by Sam Simon
Friday, Jul. 16, 2004 at 7:18 AM
Orphans on Trial. Pediatric AIDS Drugs Forced Into State Wards and Orphans - Money for Big Companies equals Big Loss for Kids. This was broken through Indymedia, and is now finally entering the mainstream.
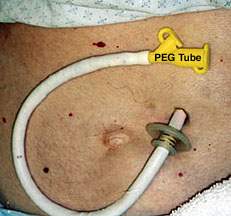
peg_tube.jpg, image/jpeg, 231x216
Orphans On Trial
Abandoned kids are force-fed experimental AIDS drugs at a Catholic children's home in Washington Heights. And the city wants it that way.
By Liam Scheff
When Christine Maggiore tested HIV-positive in 1992, her doctor told her to get ready to die. But she wasn't interested in dying.
Maggiore was told that the AIDS drugs would make her sick, so she skipped them, instead relying on natural methods to support her health. A year and a half later, she was so healthy that her doctor said there was something wrong and she should retest.
She did retest, several times. The tests came back negative, indeterminate and positive. Maggiore investigated the medical literature and found what is recounted above: HIV tests are highly inaccurate. She also discovered that there are gaping flaws in the HIV hypothesis itself.
Believing that this is the sort of thing people should know, she founded Alive & Well AIDS Alternatives, a resource for people who, like herself, want to make fully informed decisions about their health.
Since testing positive, Maggiore has had two children. Her kids, two and six years old, have never been tested. They've been raised on organic food, with a naturopathic approach to health. They're both intelligent and active. They don't take AIDS drugs. And they're not in the least bit sick. They regularly see their pediatrician, who has no medical complaints about their well-being.
And they're not alone. There are thousands of healthy HIV-positive people who don't take the drugs, who rely on natural regimens to support their immune function.
It was through Maggiore that I met Mona, whose children, Sean and Dana, have tested HIV-positive. By the state's definition, they're not actually her children; Mona is their great aunt and legal guardian. Her niece, a long-time drug user, was unable to act as a responsible mother, so Sean and Dana were remanded to state foster care. Mona took them back to raise as her own.
When I first spoke with Mona, she was stressed and nervous. Sean had twice been sent to the Incarnation Children's Center (ICC), a "home for HIV positive children" located in Washington Heights. First, as an infant, then again four years ago. And Dana was there until June.
"Why did they take her?" I asked.
"They said I was a negligent parent because I didn't want to give the drugs."
She'd been taking Sean and Dana to a naturopath. That the children were healthy didn't matter. When city agencies found out that the children weren't on the drugs, they took them away for mandatory treatment at a clinic and then transferred them to ICC. There, they were locked up and pumped full of drugs day and night.
"What drugs?"
"AZT, Nevirapine, Epivir, Zerit. All kinds of drugs."
To read through the list of drug studies either currently underway or recently concluded at ICC studies sponsored by government agencies such as National Institute of Allergy and Infectious Diseases and National Institute of Child Health and Human Development, and huge pharmaceutical companies such as Glaxo, Pfizer, Squibb and Genentech?is to take a trip through the nightmare world of pediatric drug research.
For example, the study called "The Effect of Anti-HIV Treatment on Body Characteristics of HIV-Infected Children" is looking for the causes of "Wasting and Lipodystrophy [fat redistribution]"?by using drugs known to cause wasting and lipodystrophy.
Or consider "The Safety and Effectiveness of Treating Advanced AIDS Patients between the Ages of 4 and 22 with Seven Drugs, Some at Higher than Usual Doses." The seven drugs in the study are all known to cause debilitating, potentially fatal side effects, yet they are administered at "higher than usual doses" in four-year-olds.
Then there's a study with "Stavudine Alone or in Combination with Didanosine." Stavudine plus Didanosine has killed pregnant women.
Or the vaccine study to be administered to children "12 months to 8 years" using "live chicken pox virus," even though one of the consequences of a live virus vaccine can be the disease itself.
Another measures "HIV Levels in Cerebrospinal Fluid." Cerebrospinal fluid can only be gathered from a spinal tap, a dangerous and invasive procedure.
There's even a study on HIV-negative children born to HIV-infected mothers that uses an experimental HIV vaccine.
Mona was never informed that Sean had once participated in clinical trials at ICC.
"But they're always changing the children's medications," she said.
I asked Mona how the children at ICC tolerate so many medications. She a lot of them don�t. �The ones that can�t are drugged through a tube,� she said.
�There�s a tube down their throat?� I asked.
�No� she answered, matter-of-factly, �they take the them in for surgery.�
�A surgeon puts a hole in them? Where?�
�In their stomachs,� she said. �If a child refuses drugs too many times, they take them away for the operation. I�ve seen it happen to children who refuse the medication.�
Incarnation Childrens Center is a foster home administered by the Catholic Home Bureau under the Archdiocese of New York. According to the ICC website, it was established in 1987 "to deal with the boarder baby crisis." Boarder babies are children abandoned at the hospital.
In 1992, "an outpatient clinic for HIV-positive children was established" and, with funding from the National Institute of Allergy and Infectious Diseases (NIAID), which is a subdivision of the National Institutes for Health (NIH), "the clinic became a subunit of the Columbia University Pediatric AIDS Clinical Trials Unit."
That's when ICC went from being a home for children of impoverished, drug-addicted mothers to a recipient of funds for allowing the NIH to use these HIV-positive orphans as test subjects.
The ICC webpage listed dozens of trials with AZT and Nevirapine conducted through the late 90s. The NIH site recently listed "[f]ive studies currently recruiting for drug trials," and "27 studies ongoing or recently completed"?all on children at ICC?as well as more than 200 at Columbia Presbyterian, ICC's parent hospital. The studies are sponsored by NIH subdivisions; many are cosponsored by the pharmaceutical companies that manufacture the drugs being tested. The studies use the standard AIDS drugs: nucleoside analogues, protease inhibitors and Nevirapine.
Nucleoside analogues, like AZT, work by stopping cell division. They stop the formation of new blood in the bone marrow, in some cases causing anemia and bone marrow death. They've caused death in pregnant mothers, spontaneous abortion, birth defects, liver failure, pancreatic failure, muscle wasting, developmental damage and death in children and adults. They also may cause cancer.
Protease inhibitors interfere with the body's ability to build new proteins. Since we're made of protein, protease inhibitors have pronounced effects on physical appearance and organ function. The side effects can be bizarre, grotesque and often fatal: wasting in the face, arms and legs, fatty humps on the back and shoulders, distended belly, heart disease, birth defects, organ failure?and death.
Almost all of this is found on the warning labels.
The first AIDS drug, AZT, was designed in the 60s as a chemotherapy drug for cancer patients, but it was never approved. Critics declared it too toxic even for short-term use, yet in 1987 it was pushed through for lifelong use in HIV-positive people. Although its trials were later revealed to be fraudulent, AZT remains on the market.
Finally, there's Nevirapine, which also interferes with normal cell function. In test trials, Nevirapine has caused severe liver damage and death in dozens of patients. Most die from organ failure due to drug toxicity. Nevirapine can also cause a violent skin disorder called Steven-Johnsons Syndrome?a horrifying condition in which the skin blisters and ruptures or peels off in large swaths, leaving bloody, exposed flesh.
Despite causing so many serious medical issues in the course of treatment, AIDS drugs don't even claim to work. Every AIDS drug label bears a version of this caveat:
"This drug will not cure your HIV infection. Patients receiving antiretroviral therapy may continue to experience opportunistic infections and other complications of HIV disease. Patients should be advised that the long-term effects are unknown at this time."
So why do people take the drugs? Because they test HIV-positive. But as Christine Maggiore learned, HIV tests are highly inaccurate.
Most HIV tests are antibody tests, which means that they can cross-react with normal proteins in human blood. There are nearly 70 commonly occurring conditions?as listed in the medical literature?that are known to make the tests come up positive. These include yeast infections, colds, flus, arthritis, hepatitis, herpes, recent inoculations, drug use and pregnancy.
The remaining HIV tests, called viral load tests, can produce dozens of conflicting results?even from the same blood sample.
HIV tests are so unreliable that they all bear a disclaimer: "At present there is no recognized standard for establishing the presence or absence of HIV-1 antibody in human blood," or "The AMPLICOR HIV-1 MONITOR [Viral Load] test is not intended to be used as a screening test for HIV or as a diagnostic test to confirm the presence of HIV infection," or "Do not use this kit as the sole basis of diagnosis of HIV-1 infection" (Abbott Laboratories HIV Test, Roche Viral Load Test and Epitope, Inc. Western Blot Test, respectively).
And the kicker: Positive test results can occur due to "prior pregnancy, blood transfusions...and other potential nonspecific reactions" (Vironostika HIV Test, 2003).
In short: In the 90s, drug companies like Glaxo Wellcome and Abbott Labs began recycling old chemotherapy drugs for the new AIDS drug market. This market consisted of gay men who weren't told that the HIV test was a nonspecific antibody test. They were told, however, that AIDS was an unavoidable outgrowth of testing positive on this test, and that HIV was a fatal condition.
If you look in the medical literature, you'll find that neither of these assumptions is true.MONA'S SON SEAN has lived in a virtual coma his entire life. He was put on AZT in infancy. The drug made him so sick that he couldn't swallow solid food and, as a result, he ate through a tube in his nose until he was three. He had no energy. He was constantly ill. He couldn't play or even walk without becoming exhausted. Sean got sicker every time Mona gave him the drugs, so she cut down the doses. His energy level began to improve. She continued to wean him off the drugs and started taking him to a naturopath.
"For the first time in his life," she told me, "he became a normal boy. He could play with the other children, he could walk, he could run. He smiled and laughed. He was normal."
This would've been good news, except that Sean was born to a mother who once tested HIV-positive. Sean, the recipient of his mother's antibodies, also tested positive.
The Administration for Children's Services (ACS) came down hard on Mona for not drugging him. She was sent to a new doctor, an AIDS specialist at Beth Israel, who put Sean on a "miracle drug," Nevirapine. Within six months, he was on life support due to organ failure.
That's when ACS decided that Sean should be put into ICC. They said he'd be there for four months; he was there for more than a year. Mona had to get a lawyer to get him out.
Mona showed me Sean's medical records. They told the same story: AZT, Nevirapine, the ICU.
"Now they have Dana on the drugs."
Mona introduced me to Sean on a basketball court near their home. He was a cute kid. His jacket was too big for him, and he walked with a little shuffle?and a little wariness. He was small. I have a picture of myself at four years old?oversized denim jacket, swinging my legs a bit as I walked?and I was about the same size as Sean. Except Sean was 13. He weighed 50 pounds and was about four feet tall. An AZT baby. Stunted, his cells damaged from the inside out.
Incarnation Childrens Center is housed in a four-story brick building, a converted convent with barred windows. At the entrance, there are glass panes on either side of a large, solid door with a camera above it. The day I went to ICC, there were children pushing up against the glass beside the closed door looking at me.I walked through the door and into a waiting room with a wide steel elevator door at the far end. I signed in as a family friend of Mona's. The nurses eyed me suspiciously but didn't stop me from entering.
Beyond the reception area was a large, dark room with stained-glass windows on the far back wall. Children were grouped around folding tables.
The kids ranged from a couple years old to almost adult. Except for a few Hispanic kids, they were mostly African-American. A number of the children were in wheelchairs. There was a boom box playing in the background. Somebody had brought in pizza in cardboard boxes. A young woman in sweatpants sat on one of the chairs. She looked at me and seemed embarrassed; it was her 18th birthday party. A few bored, pale teenagers sat around in the corners, watching with detached, vague expressions. They were volunteers, coming to do community service for the AIDS children.
The wheelchair-bound kids were being fed or drugged, or both, with a milky-white fluid dispensed through tubes coming out of hanging plastic packs. The tubes disappeared beneath their shirts. Their eyes were vacant, pained, focused at a point in the distance that I couldn't see.
I walked down a short hall into another room. There was a boy, maybe 10 years old, who had a bloated, water-logged appearance. He waved and shouted, motioning for me to come play with him. A childcare worker said his name sharply, like a warning, then looked at me sternly.
Back in the hallway, another little boy approached me and held out his arms. I picked him up, and he squealed and squirmed playfully. As I tried to get a better grip, my hand hit something hard?plastic. There was a piece of plastic covering a hole in his abdomen. I went cold and put him down carefully. Again, the nurses stared at me.
Getting ready to leave, I noticed a girl with a bloated stomach. She was probably 12 or 13 years old. I looked down - there was a clear, hollow plastic tube curling out of her sweatpants.
The thick, stale air was overwhelming, and it's then that I realized the windows were not only barred, but shut.
"If they were open," Mona would later tell me, "the kids would try to get out."
As I left, I again noticed the massive steel elevator door. According to Mona, it led to the clinic.
"That's where they give them the drugs. Upstairs. They used to do it down here, but they didn't like the other children seeing them give the drugs."
Dr David Rasnick is a visiting researcher at UC Berkeley whom I worked with on a series of articles examining the AIDS debate. When I told him what I'd seen at ICC, he was disturbed?but not entirely surprised.
"AIDS doctors always assume their patients are going to die," he said. "Nobody ever asks if an AIDS patient is actually sick from drug toxicity, because they never considered that the person had a chance anyway."
Last September, I requested an interview with an ICC official. A nurse told me that no one could come because "the children all have chicken pox." I remembered the live chicken pox vaccine.
I showed up anyway. They wouldn't let me in, but they gave me a brochure. It was filled with black and white pictures of patients, exactly like the children I'd seen?drugged, damaged, with tubes hanging out of them.
In the middle of the brochure was a two-page photo of a drug tray filled with syringes. The drug schedules read, "8 am, Valium, Lasix, Prednisone, Bactrim, Epivir, Colace, Nystatin, Ceftriaxone."
There was a caption below the photo: "Medicine, medicine, medicine, medicine. The medicines give you a clue of how complicated HIV disease in childhood is. Ironically, years ago, one of my old professors told me that any patient who's put on more than four drugs should find a new doctor."
In the back of the brochure, there was a photo of a man handling a small white coffin, and another of a child's coffin in the front seat of a hearse. In the back seat, an infant sat on a woman's lap. There was no mention of drug toxicities. When these children die, they just call it AIDS.
Rasnick had told me about a nurse, Jacqueline Hoerger, who'd worked at ICC in the early 90s and had an experience similar to Mona's.
Hoerger had tried to adopt two little girls from ICC to raise and care for with her husband. She administered the drugs "by the book" for about a year, and watched as the girls got sicker. She started researching the AIDS drugs. After much consultation with an open-minded M.D., she decided to give the girls a permanent "drug holiday." To her relief and amazement, the girls improved remarkably. She documented their improvement with her doctor.
When it was revealed to the adoption agency that she wasn't drugging the girls, New York Administration for Children's Services took them away and returned them to foster care. It didn't matter that they were better. It only mattered that they took the drugs.
In October 2003, I contacted ICC's executive director, Caroline Castro. She told me to write out my questions and send them in an email, which I did.
Where do the kids come from?
What's the current protocol for treating HIV-positive children?
I read on your website that you're participating in clinical trials. What kind of trials? What kind of funding do you get for participating?
Castro replied: "ICC appreciates your interest in our services but regretfully declines to participate in your project."
I called her anyway and asked her about the clinical trials. She said that ICC wasn't participating in clinical trials. When I noted that the NIH website lists ICC as a participant, she yelled at me.
"Why do you have to write about ICC?" she asked. "Don't write about us. You should write about somebody else." Then she hung up.
I called ICC's medical director, Dr. Katherine Painter. I got lucky, she agreed to speak with me. Evidently, she and Castro weren't sharing emails that day. I interviewed Dr. Painter for about an hour. Painter responded to my questions in extremely cautious, academic language.
When I mentioned the toxicity of AZT, she agreed that there had been some problems. But, she assured me, the new drugs had solved them.
According to Painter, the "biggest problem facing families with HIV-positive children is adherence." Adherence is a code word for people who don't want to take the pills. It doesn't mean illness; it means obedience to a drug regimen.
I asked her if ICC participated in clinical trials.
"Many of the clinics that refer to us are participating in clinical drug trials. Children participating in a drug trial undergo monitoring, testing and supply of an experimental drug through their outpatient clinic and we maintain that treatment here."
Had Castro lied to me? Clearly, the Incarnation Children's Center was participating in clinical trials. The kids may be enrolled at various area hospitals, but they're housed and drugged at ICC?which sounds an awful lot like participation.
I noted that the NIH clinical trial database listed hundreds of drug studies using children.
"There are loads and loads of trials going on in children," she replied.
As for adherence among the young patients, Painter noted that the drugs have a "significant, lingering, bitter taste." So they mix the pills or powders in chocolate or strawberry syrup.
But "for some cases," she said, "it's better administered through a g-tube." That's the stomach tube.
I asked her how they put in a g-tube. She said a surgeon cuts through the child�s abdomen, �through the abdominal wall musculature, and then through the stomach. It creates a very small hole, about a quarter inch. It takes several weeks to heal well, so it�s a bit tender. A small tube is placed through the stoma or opening. From the outside you can connect a syringe or feeding tube.�
I asked why ICC insisted on drugging children in this manner when there are thousands of HIV-positive individuals who aren't sick, or who are pursuing naturopathic regimens with great success.
Painter admitted that she knew about these people?she used the industry term, LTNP (long-term non-progressors). This is a title used by AIDS academics to dodge the fact that even the Center for Disease Control & Prevention agrees that the majority of people with HIV aren't sick. Most AIDS patients are given the diagnosis because of a T-cell count rather than an actual illness.
The LTNPs I know are involved in health-supportive regimens, they avoid immune-damaging practices, foods and substances?including the AIDS drugs.
"In treating AIDS," I asked, "why aren't we looking at supporting the immune system? Why are we giving people who are already sick drugs that kill the lining of the intestines and cause liver failure? Look at the adverse effects of any of these drugs?"
She interrupted. "Yes, of course, drugs have adverse reactions. But the risk/benefit of any medication must be weighed." She was becoming irritated. "May I remind you that untreated HIV infection is a terminal diagnosis."
And there it was, exactly what Dr. Rasnick had said: "AIDS doctors always assume that their patients are going to die."
But Painter had already agreed that wasn't true. There were the LTNPs. If they weren't dying and they tested positive, then her statement was incorrect.
She began to lecture me about the progression of the disease. First positivity, then, 10 years later, sickness, then inevitably, death.
"Fine," I said, "let's say that someone who tests positive is indeed ill. The kids in ICC, besides being drugged all the time, are children of chronic drug abusers. Isn't that a good reason to be sick?"
"No," she said.
"But HIV tests cross-react with antibodies produced from drug abuse."
"No," she protested.
"Yes, they do," I said. "Drug abuse, hepatitis, there are about 70 recorded conditions that make the test come up positive."
In reporting on the AIDS debate, I'd never met an HIV researcher or doctor who told me that HIV tests were even close to 100 percent accurate. Even the lab technicians I've met accept that the tests can be inaccurate and unreliable.
I ask again: "Why are we treating AIDS patients with drugs that kill their immune systems? Shouldn't we be helping them build their immunity? Shouldn't we be saying anything that works in the treatment of AIDS is valid?"
Painter said that there was room for "supplementary therapy, including nutritional support" but, she reiterated, "antiretroviral therapy has been the leading intervention that has significantly reduced morbidity and mortality in HIV infection."
I looked at my pile of papers: dozens of drug studies in which patients have died, in the researcher's own estimation, specifically because of the drugs. I looked at the warning labels: heart attack, organ failure, wasting, bone loss, anemia, birth defects, skin loss, bloody rashes, deformation and death.
Painter was in charge of at least 20 kids at a time, many of them orphans taken from their homes for the purpose of having a drug regimen enforced. She knew or was willing to admit less about HIV tests and HIV drug toxicity than almost any medical professional I'd ever spoken with. I thanked her for her time, and hung up.
Inside Incarnation Childrens Center, the children in wheelchairs stared ahead, unable to focus. I wanted to take them all outside, into the fresh air. It was a bright sunny day, and they were locked up in this room, a girl's 18th birthday party under stained glass.
I approached one of the children in a wheelchair, a boy about 12. There was something strange in his face?his head was oddly shaped. It was a bit squashed, with the eyes spaced widely. His limbs and torso were slightly warped, shortened and weak-looking. This is what happens to AZT babies.
I looked at the other children. Same arms, same legs, same faces. One boy on half-crutches tried to dance to the music. His legs dangled beneath him, his feet at odd angles to the ground. I knelt by the boy in the wheelchair. He made a slight sound, like a panic deep inside trying to get out. I didn't want to alarm him, so I got up.
I met a boy named Amir who was sitting at one of the tables. He was about six years old. Amir had a stomach tube. He had also undergone multiple plastic surgeries to remove "buffalo humps"?that's what the AIDS doctors call the large, fatty growths from the necks and backs of people who take protease inhibitors.
I walked over to him, and he smiled broadly. His head was in that same squashed shape, and his back and shoulders were oddly rounded. He grabbed onto my shirt. I knelt down and he put his arms around my neck for a hug. There were large round discolorations on his neck where the lumps had been removed. After a couple minutes, I tried to get up, but he held on. I took his hands gently in mine, held them for a moment, then carefully let go.
Five months later, Mona saw Amir in the hospital. "My stomach is swollen; it got big," he told her. "They cut me, they cut me." He pointed to an incision on his side.
"I think it's the tube," Mona told me. "I think it's infected."
When I asked Dr. Painter how they decide that the stomach tube should be used, she told me, "When other interventions to help a child take the medication by mouth have failed."
Something certainly failed with Amir. Two weeks after Mona saw him in the hospital, he was dead.
www.altheal.org/toxicity/orphans.htm